What is a Brachial Plexus Injury?
A brachial plexus injury refers to an injury to the brachial plexus (BRAY-key-el PLEK-sis), a network of nerves that provides movement and feeling to the shoulder, arm and hand.
A brachial plexus injury refers to an injury to the brachial plexus (BRAY-key-el PLEK-sis), a network of nerves that provides movement and feeling to the shoulder, arm and hand.
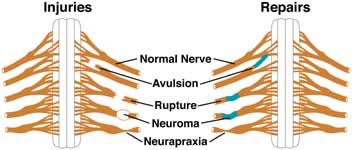
The nerve is torn away from its attachment at the spinal cord; the most severe type. An eyelid droop suggests an avulsion of the lower brachial plexus (Horner's syndrome).
The nerve is torn, but not at the spinal cord attachment.
Scar tissue has grown around the injury site, putting pressure on the injured nerve and preventing the nerve from sending signals to the muscles.
The nerve has been stretched and damaged but not torn.

Last Updated 02/2024
Learn more about our editorial policy.
3333 Burnet Avenue, Cincinnati, Ohio 45229-3026
© 2026 Cincinnati Children's Hospital Medical Center. All rights reserved.


